
AN ALTERNATIVE TO THE HIV HYPOTHESIS OF THE CAUSATION OF AIDS.
by GORDON THALLON STEWART, M.D.*
August 8, 2008
ABSTRACT
This article questions the orthodox, consensual view of a global pandemic of AIDS due exclusively to heterosexual and perinatal transmission of HIV. It offers instead an alternative epidemiological analysis of validated data and experience in the passage of time since 1982 showing that outbreaks of diseases registrable officially as AIDS in countries with adequate facilities for surveillance and djfferential diagnosis occur mainly or only in communities of homo– and bisexual men, drug addicts and their consorts who engage in or are subjected to highly communicable risk behaviours conducive to overloads of sexual and other infections, malnutrition, loss of immunity and vitality. Except in these communities, AIDS is uncommon or entirely absent. Epidemics due exclusively to heterosexual transmission of HIV never happened in the UK or in general populations of other developed countries in which AIDS is an unnatural, often self–inflicted disease, wholly avoidable or preventable in both sexes and perinatally by recognition of high risk situations and behaviours. In sub–Saharan and some other developing countries, risks are wider, diverse and probably relate to RNA and activity of other retroviruses in the human genome causing false positive reactions in serological tests and PCRs, additionally to those known to be caused by bacterial infections. But higher, direct risks arise from abuses, exploitation and neglect of women and girls, and from incalculable overlaps with lethal, indigenous diseases and disorders linked to deprivations and unmanageable 3–4 fold growth of populations since the 1960’s.
Since 1984, a prestigious and formidable official Consensus of the US Centers for Disease Control, National Institutes of Health, Agencies of the UN, all national health authorities, editors of major medical journals, official bulletins, standard text–books, examination manuals, and therefore all the main medical journals and employers of health personnel have insisted that there are epidemics of AIDS in all developed countries and that these are part of a global pandemic already proceeding in less developed countries, especially from undefined points of origin in sub–Saharan Africa and potentially in Asia, due essentially to heterosexual transmission of a putative retrovirus HIV which uniquely causes loss of immunity to common infections, incurable illness and mortality. On the basis of this (HIV) hypothesis of its origin, causation, pathogenesis and transmission patterns (1), this Consensus claims also that HIV/AIDS will not be controlled until effectives vaccine or curative drugs are discovered and used on a global scale.
All this is highly questionable, as I began to find when, in 1982, the World Health Organisation (WHO) invited me to assist them in monitoring information and data accumulating in reports in New York and California since 1981, when the diseases later registrable collectively as AIDS, were first described in 5, then 15 and within months hundreds of cases of a new, devastating, lethal illness spreading uniquely in certain communities of promiscuous homosexual men. These men, like numerous others unrecognised until 1980 – 82, were already sick with sexual and other communicable infections, notable hepatitis B. They often inhaled, injected or ingested poisonous, addictive drugs (2,3). The new disease was rigorously and accurately identified by the US CDC as a Gay–related Immune Deficiency disease (GRID) of males which could be conveyed to females by bisexual men, and to some infants perinatally. Although extremely difficult to treat, it could be avoided by recognition of risks and risk behaviours, as above, which enabled most homosexual males and almost all white females to escape it though there were immediate increases in both sexes and perinatally in drug–using black–hispanic communities in USA, including immigrants from Caribbean islands.
The same disease, renamed as an acquired immune deficiency syndrome (AIDS), began to be detected in much smaller numbers in communities of homosexual men in other cities in USA, western Europe and Australasia in 1982, and worldwide thereafter (4). Patients with AIDS also reported previous infections and frequent reinfections identifiable as gonorrhoea, herpes, varicella–zoster, papilloma and cytomegalo– viruses along with bacterial, fungal and protozoal infections causing choking cough, pneumonia, genitor–urinary and alimentary infections with intractahble watery diarrhoea, rapidly–fatal loss of appetite, weight and vitality. There was therefore, from the optimistic 1960’s onward when the damaging infections of infancy, childhood and old age were diminishing, paradoxical increases in other communicable infections as above in the usually healthy majority of adolescents and young adults. Alongside, there was a far greater recurrence of almost all the known sexually transmissible diseases (STD’s) in the Americas, Europe, Africa and SE Asia, together with some drug–resistant and new infections, especially that caused by Chlamydia, a pervasive member of a group of microbes which persisted as pelvic inflammatory disease in women, also caused ocular and pneumonic infections in children, and soon became endemic (6).
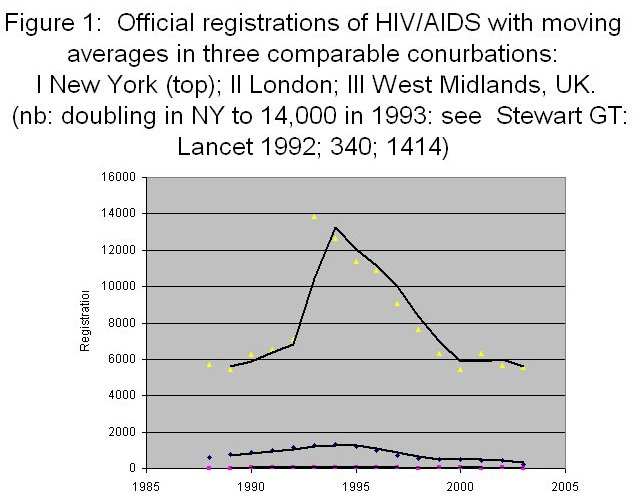
AIDS, along with misuse of drugs, was perceived in USA in 1983 as the worst of these afflictions because of its lethality and, not least, because many Gay men, outing conspicuously and cheerfully from stigmatisation and ostracism, became instant victims of these new and deadly hazards awaiting their escape and extroversion. In USA, eight of the 15 cases reported in 1981 died within a year and all the others subsequently. This mortality increased in 1983 in a fast track of thousands of cases in homosexual men and drug addicts in New York City (Fig 1), California and Florida. A few cases in celebrities in showbiz and sport attracted popular interest and charitable funding for what was increasingly publicised as a new, lethal infectious disease to which everyone might be susceptible.
The evidence that AIDS was infectious received further support in 1983 when Montagnier et al at the Pasteur Institute, the historic Mecca of virology in Paris, reported the presence in cell cultures of an excised lymph gland of a lymphopathic agent (LAV) thought to be a retrovirus. Professor Montagnier and members of the same group reported later (7) that the lymphopathic properties of the cell culture depended upon the presence of a contaminating mycoplasma but, when they sent it in 1983 to Dr Robert Gallo, leader of a more experienced team working on retroviruses as causes of cancer at the National Cancer Institute of the USA in Berthesda, Md., he and his colleagues confirmed that it yielded a retrovirus which was identical to one (HTLV III) of a lymphotropic group associated with leukaemia which he and experienced colleagues had already isolated also from homosexual men with AIDS in their area, but not from healthy controls. Antibodies to these retroviruses had been detected and the US CDC feared that HTLV III was spreading to general populations in the USA and internationally. Support for this prediction and fear of a pandemic dominated meetings convened in Geneva by the WHO in 1986–87 when LAV/HTLV III was renamed as HIV,the unique cause of AIDS. Reservations had been expressed (6) from 1984 onward, notably in 1987 by a career (and bench) expert in retrovirology, Professor Peter Duesberg of UC Berkeley (8). He agreed that the renamed retrovirus HIV had been isolated but denied that it was pathogenic and insisted that AIDS was due to recurrence of former infectious diseases and/or the use of immunosuppressive therapeutic and recreational drugs. He defended this view vigorously while AIDS expanded in USA eventually to about 800,000 registrations by 2000 and almost a millionby 2005 (>3000/mn), more than in any other developed country, mainly because of an excess in black–hispanic minorities in whom STD’s, tuberculosis, cervical cancer and misuse of drugs were endemic and increasing. AIDS had been reclassified by WHO in Africa in 1985 to include these and non–specific conditions like recurrent diarrhoea as AIDS.
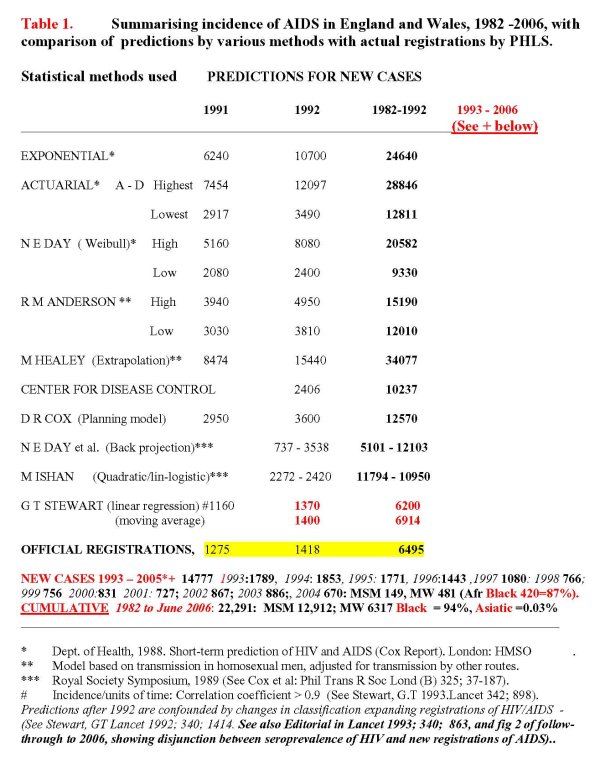
In Europe, AIDS was at first confined to major cities like London, Paris and Amsterdam. In the UK, 33 cases were reported in young homosexual males in 1983. 15 died in that year, 18 subsequently. Reports increased from about 100 in 1984 to about 1500 in 1994, decreasing thereafter to less than 700 in 2004 and, cumulatively, to about 20,000 from 1982 through 2007 in a population of 60 million (~333/mn), mainly in London. Elsewhere, it was unlikely that a medical practitioner would see many if any cases. However, during this period, mathematical models used by experts convened by the Royal Society (Table) were predicting thousands or hundreds of thousands of new cases. whereas simpler models devised by myself based on trends in risk groups through 1989 (9) gave figures which proved to be within 10% of actual registrations in the UK and also in New York City through 1992. In that year, WHO and CDC again expanded criteria for classification of all seropositives as HIV disease (= AIDS) by including cancer of the cervix, tuberculosis, persons with low CD4–lymphocyte counts and drug addicts in heterosexual registrations of AIDS.
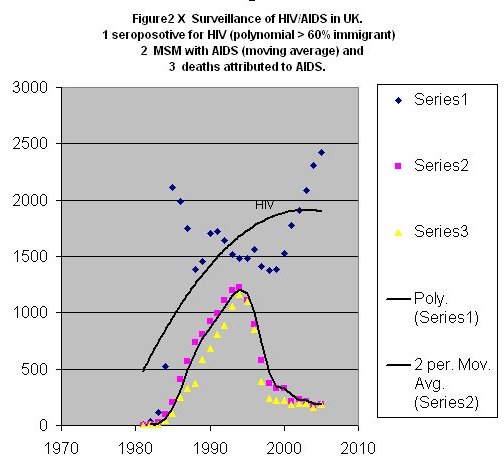
This radical reclassification led to a further 2–4 fold increase of registrations in the USA (Figure 1) but not in the UK where there were no cases in females in 1982–4 and only 50 registered cumulatively by 1989 (0.8/mn), of whom 30 were partners of bisexual men or drug addicts, while 20 were thought to have acquired AIDS from blood transfusions or surgical grafts and twelve infants born to pregnant women were thought to be at risk of AIDS. The majority of these cases were and still are in the London conurbation, with smaller proportions in Edinburgh, Brighton and a few other cities, and very few in the remainder of the UK. In most of the females, exposure to HIV/AIDS occurred overseas, often in sub–Saharan Africa, or with partners from there. About 70% all new cases are now in ethnic minorities with a significant excess in those from Afro–Caribbean countries, a much lower frequency in Asiatics, a decrease in UK residents and a continuing disjunction between asymptomatic seroprevalence of HIV and registrations of AIDS (Figure 2). A similar disjunction is now apparent in Canada but in the United States it is masked by increases of AIDS in black–hispanic residents. In Europe, the data and verifiable patterns of transmission are often constrained by political correctness, while in developing countries, especially in sub–Saharan Africa, interpretation of events is impeded by lack of, or gross inaccuracies in surveillance and projections (10) which exaggerate the frequency of AIDS but ignore the inordinate 3 – 4–fold growth in birth rates and population which in all of these countries – except South Africa – already exceeds by far domestic and international humanitarian and fiscal resource. Political correctness ensures that blame for this can be shifted to President Mbeki of South Africa who has dared to question the HIV hypothesis, and the use of external statistics and pressure by the Consensus, to mandate medication by antiretroviral drugs in his country.
With hyperactive assistance from the US Institutes of Health, and passive acceptance by medical and other health professionals, the Consensus justifies this by referring to over 100,000 publications in peer–reviewed journals endorsing an unprecedented volume of laboratory and clinical results supporting the HIV hypothesis. There is independent justification for some of this in, for instance, the successes reported for combined therapy with antiretroviral (ARV) along with other drugs in producing reductions in surrogate estimates of viral load and relief of symptoms. But their case is shattered by their uncritical acceptance of astronomical projections of a outbreaks which have recently been exposed by Dr James Chin who was chief of the section on the epidemiology of HIV/AIDS in WHO from 1987 until recently. In his book (10), he exposes miscalculations, false assumptions and ‘Titanic’ exaggerations in the projections used by UNAIDS, health authorities and journals to forecast a catastrophic pandemic comparable to that in sub–Saharan Africa throughout the Indian subcontinent and Asia. Much of this appears to be “Deliberate deception” (11). Nevertheless, and illogically, Chin accepts the hard core of the HIV hypothesis, as stated in the London (1988), Durban (2000) and later declarations and projections that AIDS has spread globally by heterosexual transmission of HIV. This will continue until a vaccine is produced for use after controlled trials assessed by surrogate tests which should differentiate viral RNA’s in the human genome. Earlier experience, for instance in the well–designed Nordic trials, in the sudden cancellation of the extensive vaccine trials organised by health authorities collaborating with the Merck company and in the total absence of a replacement all show that prevention by vaccination is not only ineffective but probably dangerous (12) and logistically impracticable (13).
Twenty–five years of these failures have had an enormous negative impact by subtracting resources required for correction of underlying deprivations like elementary hygiene and malnutrition, competing disasters like lethal infections and, above all, practical instruction on how to avoid AIDS and all the inter–related sexually–transmissible diseases. In the fiscal year 2007, expenditure on unsuccessful research and trials amounted to US $287 million from the Bill and Melinda Gates Foundation in addition to comparable or greater ring–fenced allocations in $ billions from other international sources. The main beneficiaries are big pharma companies together with recipients of big grants and exemptions from accountability and conflicts of interest. It is not surprising that they are unwilling to admit this, or to open their minds and resources to alternative approaches but it is very surprising and sinister to find in the wider forum of honest science that any alternative to this deception and mismanagement is ignored and thereby denied attention and open debate even when the extent and depth of the deception has now been revealed undeniably in sectors of the Press (12), in a book by Bauer (14) analysing huge, name–based US data –base, and in other recent books. Reviews from the Consensus (11,15–18) admit the need for structural reform in a deteriorating situation, with customary gravitas and calls for even more investment in vaccines, but give no reference to these disclosures of fundamental weaknesses in their construct and management of AIDS, or to any need for alternatives to the falsifiable dogma of the HIV hypothesis.
The main alternative is revealed by the passage of time and the availability of validated data since 1988 showing that the epidemics of AIDS caused by heterosexual transmission of HIV – the keystone of the HIV hypothesis – never happened in the UK, or in any other developed country except USA (4, 9,14). This is probably because AIDS is still disproportionately prevalent there and transmissible by high risk behaviours within communities of homosexual men and some ethnic minorities. Otherwise, it is an unnatural disease which is self–inflicted and wholly avoidable or preventable in both sexes.
This summary of plain facts is the short story about HIV/AIDS. The long story is one of error, misunderstanding, deliberate and accidental deception, avoidable suffering and deaths in the face of dedicated but often misplaced concern, health resources and expenditure.
References
- The Durban Declaration. Nature 2000: 406: 15. See also ibid 407; 286.
- Newell GR, Mansell PW, Spitz MR. Amer J Med 1985; 78; 811–6.
- Lauritsen J, Young I. The AIDS Cult. Provincetown, Asklepios: 1997.
- Weekly epidemiological reports, WHO; 1982– date. Geneva. See also HIVAIDS Surveillance Reports, USA 1982–05, revised 2007 and UK Surveillance Updates by Public Health Service Laboratories and Health Protection Agency,1982 – 08.
- Stewart GT, The epidemiology and transmission of AIDS: a hypothesis linking behavioural and biological determinants to time, person and place. Genetica 1995; 95; 173–93. See also Lancet 1995; 145; 1241, and Bull Med Ethics 1995; 106;19.
- Do, Haro S, Update on sexually–transmissible Diseases. EURO–WHO 1984.
- Lemaitre MD, Guetard Y, Henin L et al. Res Virol 1990; 141; 5–16.
- Duesberg PH. Cancer Res 1987; 47; 1199 – 1220.
- Stewart GT. Lancet 1993; 342; 898, See also Editorial 342; 863–4.
- Chin J. The AIDS Pandemic. Oxford, Radcliffe: 2007.
- Nature 2007; 447; 531–2. Time for a Change.
- See The Independent Newspaper. 24 April, 2008.Report on AIDS Vaccine..
- Stewart, GT. Arch Clin Bioethics 1999; II; 56–60. See also Craven BM et al. Economic Issues 2003; 8 (1), 1531.
- Bauer HB. The origins, persistence and failings of HIV/AIDS theory.
- El–Sadr W, Hoos D. The President’s Emergency Plan for AIDS relief – is the Emergency over? New Eng Med J 2008; www.nejm.org July 30,2008
- Steinbrook R. The AIDS Epidemic – a progress report from Mexico City. Ibid August 20, 2008.
- Gupta GR, Parkhurst JO, Ogden JA et al. Structural approaches to HIV prevention. Lancet 2008; 372; 764–75 (August 30).
- Steinbrook R. The AIDS epidemic - A progress report from Mexico City. New Eng J Med 2008; 359; 885-7 (August 28)
- Bertozzi SM, Laga M, Bautista-Arredondo, Coutinho A.. HIV Prevention Serial 5. Lancet 372; 831-846. See also Piot P, Bartos M,LarsonH,Purmima M. Serial 6. ibid; 372; 845-59 (September 6).
* Author details: The writer, Gordon T. Stewart, M.D., is emeritus Professor of Public Health at the University of Glasgow, UK, and an honorary consultant physician in epidemiology and preventive medicine in the NHS and allied agencies, UK. He was formerly a Professor at the University of North Carolina, Chapel Hill, NC, at Tulane University in New Orleans, La, a medical consultant to New York City, WHO, AMREF (Kenya), UNICEF and health authorities in North America, Europe, Africa and Asia., a former Senior Visiting Fellow of the US National Science Foundation, a Visiting Professor at Medical Colleges in India, Pakistan, Senegal, and Cornell Medical School in the New York Hospital, a founder member of Reappraising AIDS, an emeritus Fellow of the Infectious Diseases Society of America and a former member of the Editorial Board of the Journal of Infectious Diseases.